
Shoes, Orthotics & Balance
Shoes
Children’s shoes must be constructed properly and must fit properly. We check our patient’s shoes for healthy design features and for correct fit, and provide parents/ guardians with advice.
Barefoot is not best for children with joint hypermobility. Hypermobile children have much worse barefoot balance than non-hypermobile children. Barefoot exercises do not solve this issue. Barefoot exercises cause the over-used muscle groups to be further over-used. Some children become better at using the wrong muscles. This leads to early onset joint mal-alignment and/ or pain.
Hypermobile children’s balance improves immediately a properly fitted shoe is placed on their feet. These children should not be told to take off their shoes at kindergarten/ day care/ school. Their physical capabilities will be impaired if they are required to perform weight bearing physical tasks barefoot. This can be equated to asking a child who wears glasses to take them off during physical tasks.


Sometimes all that is needed is the correct shoe for your child’s feet. Shoes have many combinations of characteristics, such as the point at which the shoe first bends, the shape of the last (curved/straight), the shape of the toe-off area of the sole, the type and location of the arch support, the size of the shoe, the depth of the toe box, whether it is a sandal, boot or shoe. The cost, brand and material are not such important issues. Within brands, you will find shoes that vary considerably in characteristics. You could buy expensive shoes that will cause gait problems for your child or you can pay a very small amount for a shoe that will enhance your child’s gait. This is where professional advice is very important. As a test, go into a shoe shop and try to bend a selection of shoes. You’ll notice that some bend at the ball of the foot, others bend in the middle, and others don’t bend at all.
Flat Feet

Twisted Feet

These are examples of foot conditions that children will not grow out of. Professional intervention is required
Hypermobile Joints

Before

After (with orthotics)
ORTHOTICS
Dr Henry Netscher wrote an entire chapter in his PhD on the use of foot orthoses for children.
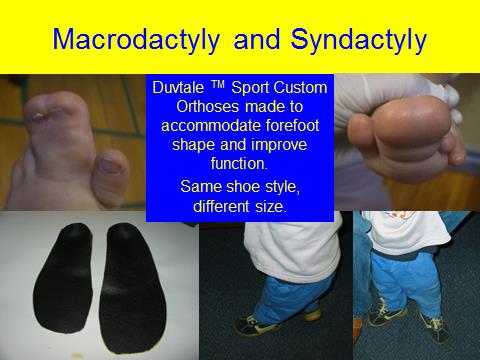
Orthotic devices made at Footlink-kidsfeet simply customise the inside of the shoe to your child’s foot.
A custom-made in-shoe orthotic may be required to improve the proprioceptive information from the feet (base of support of the body) to the brain.
At Footlink-Kidsfeet we make Duvtale foot orthoses according as designed by Dr Netscher. This orthotic was designed to treat children with joint hypermobility. It is the only orthotic designed specifically to treat joint hypermobility, and is the only orthotic design to have had its effect tested on balance control of hypermobile children. The orthotic immediately improves the proprioceptive information to the brain. The orthotic device must be housed in a shoe that is constructed properly. Off- the shelf shoes are suitable.
Dr Netscher has designed many other forms of foot orthoses to treat various other conditions.
A benefit of bringing your child to Footlink-Kidsfeet is having access to Dr Netscher’s creativity, problem solving abilities and ability to make what he designs in his on-site orthotic laboratory.
We make orthoses from plaster casts of your child’s feet. The casting process is not painful, and many children enjoy the process. We call it “foot craft”.
In general, a pair of orthoses will last a child for 1 year. The orthotics can be transferred into the next shoe size.
If however your child has a very complicated foot problem we may need to update the orthoses within the year. This is not common.


Exercises
To improve the brain’s organisation of muscles involved in control of posture, balance and co-ordination exercises will be prescribed for your child.
For vary small children (under 3.5 years) these exercises involve play related activities that challenge balance.
For children aged 3.5 years to approximately 8 years, the exercises will involve gross motor skill tasks and sensory integration tasks, involving jumping and landing with the feet in different positions and throwing and catching.
For children over 8, in general, the exercises will be more formal in order to target the specific areas in need of rehabilitation.
For many children, running drills will be prescribed. We like to help kids run faster.


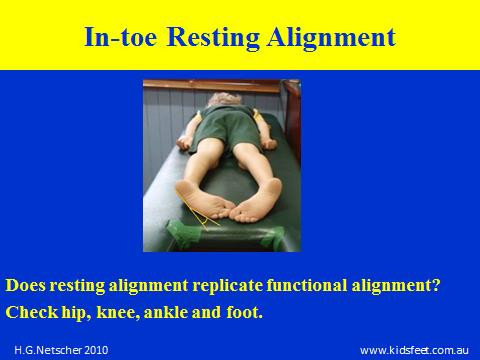
Turned in Feet from Birth
Some babies are cramped for space in-utero. This is a common cause of turned-in feet from birth.
The outside border of the foot should be straight. An easy way to determine whether their is a problem is to place a biro along the outside border of the foot. You will be able to see if the foot curves away from the biro.
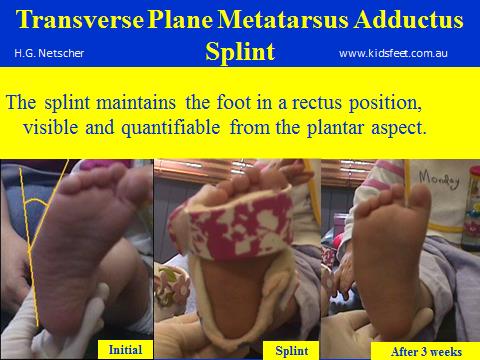
If the foot can be straightened with gentle pressure, this is called ‘metatarsus adductus’.
Dr Netscher designed the transverse plane metatarsus adductus splint to treat this problem. This splint is used when the problem is due to tightness of the muscle that runs along the inside of the arch of the foot (abductor hallucis) and over-lengthening of the muscle that runs along the outside border of the foot (abductor digiti minimi). The foot is curved because of the imbalance between these two opposing muscles. The splint is designed to restore the normal resting length to these muscles, thereby resulting in a straight foot.
The infant requires review when walking begins because the brain may recruit abductor halluces to control balance. If this is the case we need to change this early in order to avoid the foot becoming in-turned again. The child may need Duvtale foot orthoses inside straight lasted shoes in order to send clear balance information to the brain so that the brain recruits the muscles properly. In addition to this, the child may need to wear night splints if their sleeping position maintains their feet in a mal-aligned position.
The younger the child the easier, quicker and cheaper it is to treat this problem.
Before Treatment
After Treatment
Over (high)-riding and under (low)-riding Toes
Due to in-utero compression, some children are born with crooked toes. It is very easy and inexpensive to treat this problem when children are babies and infants. Often taping the toes into alignment will resolve the problem very quickly.
If left untreated, it will take much longer to bring the toes into alignment. Also, it is common that the child may develop other problems such as bunions due to the mal-aligned toe.

Before Treatment

After Treatment

BALANCE
A simple test to determine whether your child has a balance problem is to ask them to stand on one foot and close their eyes. An 8 year old child should be able to stand still on the one foot with the eyes closed for at least 10 seconds. This indicates that the proprioceptive system is sending clear information to the brain from the base of support.
If the child is wobbling and/ or loses balance within 3 seconds, there is a proprioceptive information issue. We recommend that you bring your child to have this assessed.
If your child is under 4 do not attempt this test, but note whether your child is cautious, falls often, wants to be carried often, is a restless sleeper.
Also check whether your child takes short steps when walking on soft or unstable surfaces, looks down (using the visual information to compensate for the unclear proprioceptive information), holds their hands/ arms out to the side to stabilise themselves. These are all indicators of poor balance in small children.

Some children have poor balance and are clumsy. This is because the nerve messages from their feet are not being transmitted to the head efficiently. This can be treated at Footlink Podiatrists. Children who have poor balance look down, put their arms out and take very small steps when performing very simple balance related activities.
Clawing of toes
Clawing of the toes indicates that the foot is unstable. This is generally due to joint hypermobility. The long toe flexor muscle (flexor digitorum longus) is being used by the brain to grasp at the ground and keep the joints of the foot together. This results in the toes being flexed at propulsion rather than being straight rigid levers. Clawing of the toes means over-use of the toe flexors, and under-use of the muscles that keep the toes straight in propulsion (lumbricales).
If the child continues to claw the toes this can result in toes that remain clawed at rest.
If you notice your child clawing their toes, make an appointment.

Adolescent foot: untreated claw toes
Untreated clawed toes can lead to blisters, corns and callouses. This can require regular visits to the Podiatrist to have the corns and callouses removed.

Bowed Legs
First it is necessary to diagnose whether the legs are actually bowed or whether the alignment disorder is reducible and due to muscle imbalance (pseudo-malleolar in-torsion).
We treat the muscle imbalance with night splints to improve the muscle resting length problem, foot orthoses to provide clear balance information to the brain while walking, and exercises.

Before Treatment

After Treatment

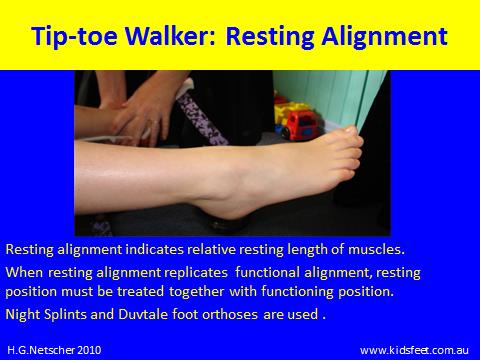
Tip Toe Walking
Tip-toe walking is one of the most complicated posture control disorders to treat. This is because the brain is referencing balance to the ball of the foot, not the entire foot. Also, the brain is recruiting the calf muscles in the opposite order than is normal. The longer a child tip-toe walks the greater the damage to the foot itself and the more likely it is that the child will not attain their gross motor skill milestones in particular independent patterning of arm and hip movement.
It is not normal for children to spend time walking on their tip-toes.
The heel should contact the ground first in walking after the infant has 90 days of walking experience.
Metatarsus Adductus

Before Treatment
